TARGET AGE GROUP: school-aged children
PUBLISHERS: UNESCO, UNFPA, Advocated for Youth
UN AGENCIES: UNESCO, UNFPA
CONTRIBUTOR: SIECUS
HARM SCORE: 15 OUT OF 15
DISTRIBUTION: Africa
Direct Quotes from the Publication
This publication received a Harm Score of 15 out of 15 (click here to see analysis). To learn more about the Harmful Elements commonly found in CSE programs or the 15 Harmful Elements Analysis Tool click here.
Sexualizes Children
- “… babies, children, adolescents, adults, and the elderly— are sexual beings.” (p. 79)
- “Children are sexual even before birth.” (p. 79)
- “Males can have an erection while still in the uterus, and some boys are born with an erection. Infants touch and rub their genitals because it provides pleasure. Children can experience orgasm from masturbation although boys will not ejaculate until puberty.” (p. 79)
- “Adolescents sometimes need help understanding that sexual fantasy is normal …” (p.86)
- “Find ONE illustrative learning objective for the following topics for the indicated age range: Sexual and Reproductive Anatomy and Physiology, ages 5–8” (p. 42)
- “Erection: The penis filling with blood and getting larger” (p. 148)
- “SAMSON and ELIZABETH: Samson and Elizabeth are classmates at university. They have been dating for a few months and are very attracted to each other. They are deeply in love and agree that they want to have sex. After agreeing to use a condom, they have sexual intercourse and both enjoy it.” (p. 273)
- “MARIE and WILLIAM: Marie and William have had sex once before. Tonight, William tells Marie that he has wanted her all day. Marie would rather just hang out and talk, but she thinks since they did it once, there is no going back. When William starts to take off his clothes, Marie says nothing to him and they have sex again.” (p. 273)
- “EMMA and SYMON: One evening Emma drank a lot. Symon finds her lying on the bed passed out. He takes off her clothes and has sex with her. She doesn’t wake up.” (p. 273)
- “KEY MESSAGES OF LESSON: There are important criteria to consider when deciding whether and with whom to be sexually active. There are many perspectives to consider when making an important decision, like whether or not to be sexually active.” (p. 276)
Note: The “key message” conveyed here does not discourage children from having sex, instead, it just tells them they have the right to make their own decisions about their sexual activity. It doesn’t set abstinence as an expected standard, nor does it help children understand the downside of early sexual activity.
Teaches Children to Consent to Sex
- “Find ONE illustrative learning objective for the following topics for the indicated age range: Communication, Refusal, and Negotiation Skills, ages 12–15” (p. 41)
- “LEARNING OUTCOMES: By the end of this lesson learners will be able to: Identify the skills they will need to be able to negotiate a safe and comfortable sexual relationship.” (p. 274)
Note: While this module does not have as strong a focus as most CSE programs have on teaching children “consent” and how to negotiate sexual encounters, it does provide several role pays depicting this kind of negotiation, including scenarios where children either ask their partner to have sex or agree with their partner’s request to have sex.
Normalizes Anal and Oral Sex
- “This is one of humanity’s most common behaviors. It is a behavior that may produce sexual pleasure and that often ends in orgasm in females and males. It may also result in pregnancy and/or STIs. In programs for youth, discussion about this is often limited to penile–vaginal intercourse. However, youth need accurate health information about all forms of sexual intercourse—vaginal, oral, and anal.” (p. 89)
- “20 Sample Questions: What does oral sex mean?” (p. 249)
- “If having vaginal sex, ensure that the vagina is lubricated or if having anal sex, that the anus is lubricated so that the condom will not break or tear. Use additional lubricant as needed, but never use oil–based lubricant, as it will cause the condom to break.” (p. 262)
- “MYTH: You don’t need a condom if you’re having oral sex. TRUTH: Actually, HPV, gonorrhea, chlamydia, herpes, and HIV can be passed on by oral sex. You can protect yourself with a condom (worn on the penis for a male receiving oral sex or cut into a sheet for a female receiving oral sex).” (p. 264)
Note: According to a 2017 article called “Receptive Anal Intercourse and HIV Infection,” published in the peer-reviewed World Journal of AIDS[1], “more cases of HIV infection have been attributed to the transmission route of AI [anal intercourse] than to any other route of transmission . . . Condoms alone only partially reduce the high risk …When one or both partners are infected with a sexually transmitted disease (STD), even with condom use, the risks are very high.” In light of these startling medical facts it is unconscionable that UNESCO and UNFPA are publishing material that would tell children “you can protect yourself with a condom” instead of telling children to avoid all sex, including anal sex, until they are married. With regard to oral sex, imagine a teacher instructing his female student to cut a condom open and insert it in her mouth while having anal sex and to expect that she will be fully protected, especially in Africa where HIV infections rates are the highest!
[1] Lavoie, G. R. and Fisher, J. F. (2017). Receptive Anal Intercourse and HIV Infection. World Journal of AIDS, 7(4), 269-278.
Promotes Homosexual/ Bisexual Behavior
- “Diversity is a fundamental characteristic of sexuality.” (p. 11_)
- “Same–gender sexual behavior is common at this age.” (p. 79)
- Stages of Adolescent Development Activity Sheet: “Sexual orientation nearly secured” (p. 104)
“With Whom Would You Disclose If You…? Were ever in a sexual relationship with someone of the same gender [or] Were ever in a sexual relationship with someone of a different gender” (p. 235)
“Sydney and Grace are alone at one of their houses. Sydney is drunk and slurring words and then lies down on the floor. Grace, who also had a bit to drink, lies down too. Feeling uninhibited, she takes the initiative and performs oral sex. Sydney feels confused and is not sure what to say. Sydney is not sure what to think since they didn’t talk about it before Grace did that.” (p. 272)
“[Teacher’s Note: If you are able to explore same–sex relationships, it can be a great teaching opportunity to make the names of the two characters in either scenario the same gender.] This can normalize relationships between gay, lesbian and bisexual people and reinforce that everyone, no matter their sexual orientation, deserves to be in a healthy relationship. If your leaners express the opinion that two people of the same gender being in a romantic relationship with each other is never a healthy choice, it’s important to point out that, although people have differing beliefs about the rightness or wrongness of gay and lesbian relationships, any two people’s relationship can have healthy or unhealthy characteristics, such as those listed on the handout. Some gay and lesbian relationships are healthy and some are not, just like some heterosexual relationships are healthy and some are not. Redirect the conversation by explaining that the point of the lesson is to give learners tools to evaluate the health of their own relationships.” (p. 281)
- “Is the material appropriate for use with learners of all races, genders, sexual orientations, ethnic and cultural backgrounds, and learners with disabilities?” (p. 296)
- “Sexual Orientation—A person’s sexual orientation is defined by their primary attraction to people of the other gender (heterosexuality) or to the same gender (homosexuality) or to both genders (bisexuality). Sexual orientation begins to emerge by adolescence.” (p. 82)
Teaches Children About Sexual Pleasure
- “—the right to pleasure, to sexuality information, to choose if and whom to be intimate with…” (p. 78)
- “This is one of humanity’s most common behaviors. It is a behavior that may produce sexual pleasure and that often ends in orgasm in females and males.” (p. 89)
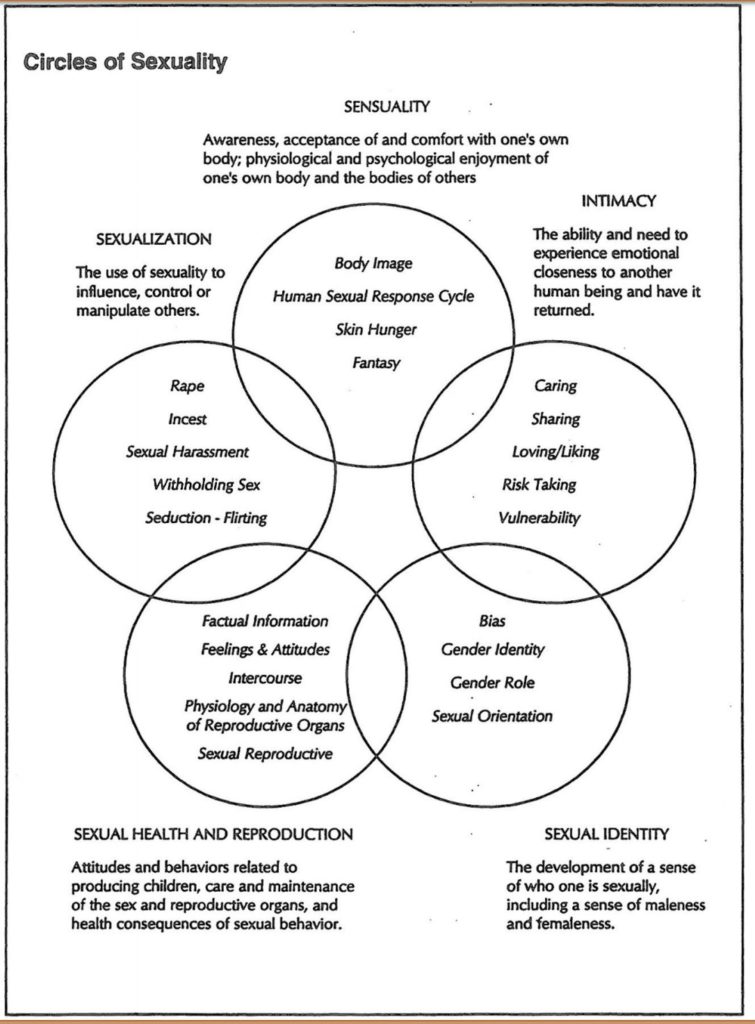
- “RESOURCES NEEDED … Five pre–written flip charts, each with one empty circle and the following as titles for the circles: 1. Sensuality 2. Intimacy 3. Sexual identity 4. Sexual health and reproduction 5. Sexualization” (p. 75)
- “Female Part – CLITORIS… Provides sensation (has many nerve endings)” (p. 139)
- “VAGINA … Provides sensation (has many nerve endings especially in the outer third) … 3” long when not aroused, 5–6” when aroused…” (p. 138)
- “Penis – Provides sensation (has many nerve endings) The average penis measures 3–4” when it’s not erect (flaccid) and 5–7” when erect.” (p. 137)
- “Most women are able to have pleasurable sexual intercourse and to experience orgasm for their entire lives.” (p. 80)
- “Some people find that the female condom decreases pleasure with sex.” (p. 168)
Promotes Solo or Mutual Masturbation
- “School–age children may play sexual games with friends of their same sex, touching each other’s genitals and/or masturbating together.” (p. 79)
- “Masturbating with one’s same–gender friends and looking at or caressing each other’s genitals is common among preadolescent boys and girls.” (p. 79)
- “Once a boy starts making sperm during puberty, his testicles never stop. So, even if he masturbates frequently, it is not possible for his body to run out of sperm.” (p. 155)
- “Masturbation is a normal part of sexual expression for most people. It will not cause a person to go crazy or blind. Many people of all ages masturbate, although some don’t because it goes against their values. You’re normal if you do it and you’re normal if you don’t.” (p. 155)
- “20 Sample Questions: Is it okay to masturbate?” (p. 249)
- “Masturbation is a normal part of sexual expression for most people. It will not cause a person to go crazy or blind. Many people of all ages masturbate, although some don’t because it goes against their values. You’re normal if you do it and you’re normal if you don’t.” (p. 155)
Eroticizes Condom Use
- “HOW DOES THE FEMALE CONDOM HELP ME? • Can be put on as part of sex play” (p. 168)
- “MYTH: Condoms make me less sensitive. TRUTH: Using a condom doesn’t have to spoil the moment. They can make some men last longer before they come, which is good news for both partners. There are lots of different sizes, shapes, colors, textures and flavors of condoms, so enjoy finding the one that suits you both best.” (p. 263)
- “If appropriate, sample male and female condoms for demonstration purposes” (p.258)
- “HOW DOES THE CONDOM HELP ME? Can help relieve early ejaculation. • Protects against HIV and many other Sexually Transmitted Infections.” (p. 170)
- “When the penis is erect, squeeze the tip of the condom and place it over the head of the penis with one hand while you unroll the condom over the length of the penis with the other hand. Make sure penis is covered completely.” (p. 262)
- “On the board, create four columns and write “well ahead of time,” “immediately before,” “during sex,” and “after sex,” at the top of each column.” (p. 259)
- “Male and female condoms are currently the only method that provides dual protection (protection against pregnancy and STIs, including HIV).” (p. 261)
- “MYTH: Condoms break easily. TRUTH: No they don’t. To avoid a condom breaking, you need to put it on carefully and make sure there’s no air bubble at the end. Be careful of sharp nails, jewelry or teeth. If the condom won’t roll down, it’s the wrong way round. Throw this condom away and start again with a new one as there could be semen on the tip of the previous condom. If a condom breaks and you’re not using any other contraception, go to a health center as soon as possible and ask about emergency contraception.” (p. 263)
- “Remember, the condom protects you from Sexually Transmitted Infections and HIV. Always use condoms to protect yourself!” (p. 170)
- “No method of birth control is 100% effective, but the condom is 85-98% effective if you use it correctly.” (p. 170)
- “Condoms are a safe and effective birth control method. • There are no serious problems when using condoms.” (p. 170)
Promotes Early Sexual Independence
- “It’s normal and healthy for boys and girls to have sexual feelings, however it’s important for everyone to think seriously about what they want to do and not do when it comes to acting on those feelings. Sexual intercourse at an early age often leads to confusion, guilt, regret, and sometimes even unplanned pregnancy and STIs, including HIV. For these reasons, it’s best to wait until you’re older to start having sexual intercourse.” (p. 155)
Note: When is older?
- “Young people around the world have many different reasons for deciding whether and when to become sexually active. Some young people wait until a certain age, until they meet someone that they feel ready to start an intimate relationship with, or until they are engaged or married.” (p. 275)
Fails To Establish Abstinence As The Goal
- “20 Sample Questions: Is it okay for a 16 year–old have had sex?” (p. 249)
- “20 Sample Questions: Do you think having sex before marriage okay?” (p. 249)
- “Many young people consider how they feel about their relationship only when they weigh the decision about whether to become sexually intimate with their partner. Some people want to make sure they have reached the legal age of consent, which is (INSERT AGE HERE) for our country. This activity will help you to think about how maturity, self–awareness, and communication skills can affect your sense of readiness to become sexually active. It will also help you identify what is most important to you.” (p. 275)
- “KEY MESSAGES OF LESSON: 1) There are important criteria to consider when deciding whether and with whom to be sexually active. 2) There are many perspectives to consider when making an important decision, like whether or not to be sexually active.” (p. 276)
- “Please review the following advice for helping decide if and when to become sexually active.” (p. 277)
- “IN DECIDING WHETHER TO BECOME SEXUALLY ACTIVE, MY ADVICE TO YOU IS THAT IT WOULD BE IMPORTANT TO… Feel close to the other person; Feel that you and the other person have made the decision together and that both of you want to have sex; Feel comfortable talking with the other person about condom use; Feel sexually attracted to the other person” (p. 277)
Promotes Gender Confusion
- “Find ONE illustrative learning objective for the following topics for the indicated age range: The Social Construction of Gender, ages 12–15” (p. 42)
- “The three pieces of sexual identity are gender identity, gender role, and sexual orientation. Each is important.” (p. 82)
- “Gender Identity—Knowing whether one is male, female, neither, or somewhere in between. Most young children have a sense of their own gender identity by as early as age two. Sometimes, the sex a person is assigned at birth is not the same as their gender identity—this is called being transgender. • Sometimes people use the acronym “LGBT” when referring to individuals of diverse sexual orientations or gender identities. L stands for “lesbian,” G stands for “gay,” B stands for “bisexual,” and T stands for “transgender.” • “Transphobia” is a term that refers to the negative feelings about and actions toward transgender people, which can lead to feeling devalued, unsafe, and isolated. Transphobia also affects the person who holds this bias and hatred because it narrows and limits the ways in which they can interact with and enjoy other people.” (p. 82, 88)
- “RESOURCES NEEDED…Five pre–written flip charts, each with one empty circle and the following as titles for the circles: 1. Sensuality 2. Intimacy 3. Sexual identity 4. Sexual health and reproduction 5. Sexualization” (p. 75)
Teaches Abortion/ Contraception
- “Planned Parenthood clinics, and many state and local health departments, hospitals, community health centers, and independent clinics offer confidential services. Some services offered by these clinics include: …Safer sex counseling… Prescriptions for birth control . . .Administering Depo-Provera (the shot) or inserting an IUD … Counseling about abortion and abortion services.” (p. 193)
- “The pregnancy does not begin until the fertilized egg implants in the uterus.” (p. 160)
- “Take Emergency Contraception (EC) right away. EC can prevent pregnancy up to 5 days after sex, and it works better the sooner you take it.” (p. 166)
- “If your last shot was more than 16 weeks ago, take Emergency Contraception (EC) right after unprotected sex. EC can prevent pregnancy up to 5 days after sex, and it works better the sooner you take it.” (p. 166)
- “WHAT IF I STOPPED USING A FEMALE CONDOM AND HAD UNPROTECTED SEX? WHAT IF THE FEMALE CONDOM BREAKS DURING SEX? • Take Emergency Contraception (EC) right away. EC can prevent pregnancy up to 5 days after sex, and it works better the sooner you take it.” (p. 168)
- “If the condom breaks during sex, the male should pull out immediately and the couple should consider using emergency contraception to prevent pregnancy.” (p. 262)
- “With Whom Would You Disclose If You… Or your partner had ever had an abortion” (p. 235)
- “The pill is very safe. Serious problems are rare.” (p. 166)
- “No method of birth control is 100% effective, but birth control pills are 99% effective if you take them each day.” (p. 166)
- “… Depo is 99% effective if you get your shots on time.” (p. 167)
- “The shot is very safe. Severe problems are rare.” (p. 167)“
- … a female condom is 79-95% effective if you use it correctly.” (p. 168)
- “Female condoms are a safe and effective birth control method. There are no medical risks. A female condom may break or slip during sex; if this happens, take EC right away.” (p. 168)
- “Some people find that the female condom decreases pleasure with sex.” (p. 168)
- “The implant is safe and effective birth control. Once you have it, it works on its own – you don’t have to do anything” (p. 169)
Promotes Peer-to-Peer Sex Ed/Sexual Rights Advocacy
- “Teens’ Rights to Reproductive and Sexual Health Services” (p. 193)
- “What are my rights to birth control, HIV and STD testing, and privacy?” (p. 193)
- “Identify potential areas for legal reform and advocacy to support young people access sexuality education” (p. 301)
- “Explore the different outcomes for young people as a result of legal frameworks and their impact to CSE and SRH services for young people” (p. 301)
Undermines Traditional Values and Beliefs
- “Are the instruction and materials used in the classroom free from the teaching or promotion of religious doctrine?” (p. 296)
- “It’s also important to change social norms and harmful practices that are not in line with human rights and increase vulnerability and risk…” (p. 57)
- “Sexuality education provides opportunities to explore one’s own values and attitudes and to build decision–making, communication and risk reduction skills about many aspects of sexuality.” (p. 11)
- “Sexuality education encourages young people to explore their values and be able to communicate these to others.” (p. 59)
- “Do not impose your personal values.” (p. 245)
- “Explore a range of values.” (p. 245)
- “Is there certainty that the speaker does not use fear–based educational techniques?” (p. 296)
- “Values can change over time, owing to changing circumstances, etc. This may have an effect on a relationship” (p. 291)
- “another key element to teaching sexuality education is to reflect on one’s own values about sexuality. To do this, let’s first explore what values are.” (p. 92)
- “Your values are things you have chosen freely—no one else can force you to choose your values, although your family and others can certainly influence you.” (p. 92)
- “Now ask teachers: Where do you think we get our values? (Answers could include family, religion, culture, and friends) . . .What is one example of a value your family feels is important? Does anyone have an example of a religious value you hold and have been taught? Which of your values come from your culture? What is a value that is widely held in this country that may be less important in other countries? Can you think of a value someone else has that you do not share? What is it?” (p. 94)
- “… a key element to teaching sexuality education is to reflect on one’s own values about sexuality. Doing so is important because while we may feel very strongly about certain things related to adolescents and sexuality, as teachers delivering sexuality education in schools, the goal is not to impose individual values on learners but rather to educate with age-appropriate information and skills.” (p. 94)
- “Part of sexuality education is enabling learners to assess and become more aware of their own values as they evolve, but it is not the teacher’s role to tell them what values to adopt. … issues around sexuality can incite strong feelings driven by our values. However, personal values about sexuality and young people need to remain just that, personal. Taking the time to examine one’s own values is important….” (p. 96)
- “When discussing values related to sexuality, the goals of the educator are to: Promote the value of respect for differing opinions…Promote universal values. Tips: Do not impose your personal values. (If you make a rare exception and share a personal opinion, surround it with comments that validate alternative viewpoints.)” (p. 243)
- “Explore a range of values.” (p. 245)
Note: The way this module handles values is the way most CSE programs do. One the one hand it says the teacher can’t share his values, one the other hand it tells the teacher to explore a range of values and to even promote “universal values.” They don’t want the teacher to pass on what may be more traditional values about teen promiscuity or transgenderism or homosexuality, etc. Instead, they want teachers to present and “anything goes” approach when it comes to sexuality. In fact, the teacher is to support and even encourage the students in doing whatever they want to do sexually, as long as they use a condom. Notice also the subtle way the materials get children to question their own or their family’s values.
Violates or Undermines Parental Rights
- “Teens’ Rights to Reproductive and Sexual Health Services -What are my rights to birth control, HIV and STD testing, and privacy?” (p. 193)
- “Consent laws requiring a parent or caregiver’s consent to HIV testing can also complicate access to testing and treatment for adolescents in particular.” (p. 203)
- “Schools and educational institutions where children and young people spend a large part of their lives are an appropriate environment for young people to learn about sex…” (p. 58)
- “sexuality education itself is grounded in a rights–based approach in which values such as respect, acceptance, tolerance, equality, empathy, and reciprocity are inextricably linked to universally agreed human rights. It is not possible to divorce considerations of values from discussions.” (p. 59)
Refers Children to Harmful Resources
- “Identify a health care provider from a local health center or hospital who can speak about the family planning and reproductive health care services” (p. 293)
- “At what age can young people access services on their own?” (p. 295)
- “20 Sample Questions: How can you get an appointment to see about contraception?” (p. 249)
- “Where is your clinic located? How can a young person get to your clinic location? Is there transportation available?” (p. 295)
- “There are community resources that can provide reproductive health care for young people.” (p. 295)
- “List three reproductive health care services that young people can get from this organization…” (p. 297)
- “Identify one place where young people can get condoms in your community” (p. 297)
- RECCOMENDED PROVIDERS OR CURRICULA
- “International Planned Parenthood Federation. Exclaim! Young People’s Guide to Sexual Rights: An IPPF Declaration. http://www.ippf. org/resource/Exclaim-Young-Peoples-GuideSexual-Rights-IPPF-declaration” (p. 342)
- “. . . permission to adapt from Family Life And Sexual Health (F.L.A.S.H.) Curriculum of King County.” (p. 5)
- “Future of Sex Education Initiative, a project of Advocates for Youth, Answer, and SIECUS” (p. 5)
- “. . . let’s go a little deeper into understanding the types of content included in sexuality education by reviewing a key resource developed by UNESCO and other UN partners, the International Technical Guidance on Sexuality Education.” (p. 39)
- “Distribute the Ministerial Commitment on Comprehensive Sexuality Education and Sexual and Reproductive Health Services for Adolescents and Young People in Eastern and Southern African. Explain that stakeholders from the Ministers of Education and Health from 20 countries” (p. 44)
- “Planned Parenthood clinics, and many state and local health departments, hospitals, community health centers, and independent clinics offer confidential services. Some services offered by these clinics include: … Counseling about abortion and abortion services” (p. 193)
- “Advocates for Youth … Amplify An online youth activism hub with information, resources, and advocacy opportunities…” (p. 194)
- “Advocates for Youth Sex Education Resource Center for Professionals.” (p. 299)
- “Planned Parenthood Federation of America, Inc. … website provides tool for teachers in support of implementing sexuality education, program evaluation tools, and additional resources. It provides information on what sexuality education is, why it is important, and how it is effectively implemented.” (p. 299)
- “Rutgers Answer … offers resources for purchase for sexuality educators, including online workshops, webinars, lesson plans, and other resources. Geared to a U.S. audience, much of the materials can be adapted to other country contexts.” (p. 299)
- “The Sex Ed Library by SEICUS … This website serves as a clearinghouse of sexuality education resources, providing links to lesson plans available online from multiple sources. Topics include human development, sexual health, relationships, society and culture, personal skills, sexual behavior, and other resources.” (p. 299)
- “Advocates for Youth. Rights, Respect, Responsibility: A K–12 Sexuality Education Curriculum. http://advocatesforyouth.org/3rscurriculum” (p. 342)
- “We would like to thank UNESCO and UNFPA staff” … “UNFPA and UNESCO teams in South Africa” (p. 5)
Other Resources
Related Family Watch Policy Briefs:
- Comprehensive Sexuality Education: Sexual Rights vs. Sexual Health (FWI Policy Brief)
- International Planned Parenthood Federation & Children’s “Right” to Sex (FWI Policy Brief)
- Abort Planned Parenthood: End Their Empire of Abortion, Deception, Fraud, and the Sexualization of Children (FWI Special Report)
- The Special Rapporteur on the Right to Education (FWI Policy Brief)
- The International Guidelines on Sexuality Education (FWI Policy Brief)
- Protecting Children and the Family from the Global Sexual Rights Revolution (FWI Presentation)



“Stop CSE!”
SIGN THE ONLINE PETITION
Please sign the petition calling upon teachers, school administrators and government bodies at the local, state, national, regional and international levels to immediately stop promoting and funding harmful comprehensive sexuality education (CSE). READ PETITION >
WARNING: This page may contain explicit and disturbing examples from CSE materials.
Regional Module for Teacher Training on Comprehensive Sexuality Education for East and Southern Africa | Child Harm Level: Extremely High
TARGET AGE GROUP: All School-Age Children
CONTAINS Harmful Elements
PROMOTES Gender Confusion
PROMOTES Contraception & Abortion
UNDERMINES Parental Rights
UNDERMINES Traditional Beliefs & Values
HAS Planned Parenthood Ties
Regional Module for Teacher Training on Comprehensive Sexuality Education for East and Southern Africa constitutes an assault on the African family and especially on the health and innocence of Africa’s children by radical American organizations. This module is part of an agenda designed to change the gender and sexual norms of countries in Africa, by promoting, among other things, promiscuity, sexual pleasure, homosexuality, and transgenderism as rights for children. It is highly disturbing that two UN agencies, UNESCO and UNFPA, would partner with such a radical group as Advocates for Youth, a sexuality activist group with strong ties and support from Planned Parenthood, and that the UN would give its stamp of approval on such harmful sexual propaganda.
QUICK LINKS: Harmful Elements Analysis | Evidence of Failure | Examples of Harmful Content
Harmful Elements
The “Regional Module for Teacher Training on Comprehensive Sexuality Education for East and Southern Africa” encourages exposing children and youth to multiple harmful concepts, through statements and various activities, such as role plays, games, and videos that are harmful and sexually engaging to children.
Examples of Harmful Content & Activities:
"Sexualization: The use of sexuality to influence, control or manipulate others.”
(Regional Module for Teacher Training on Comprehensive Sexuality Education for East and Southern Africa, pg. 123)
Circles of Sexuality Activity: